If you have been reading about stem cells, you have probably come across two sources mentioned more than any other: bone marrow and fat tissue. Both contain mesenchymal stem cells, but the comparison between bone marrow vs. adipose stem cells reveals meaningful differences in how many cells each source provides, how they are collected, and how they behave in the lab. This guide breaks down those differences so patients and providers can make informed decisions about tissue banking options.
TLDR: Both bone marrow and adipose (fat) tissue contain mesenchymal stem cells (MSCs), but they are not identical. Fat tissue yields roughly 100 to 1,000 times more MSCs per gram than bone marrow and is collected through a less invasive procedure. Published research shows differences in proliferation, differentiation tendencies, and signaling profiles. No MSC-based therapy from either source is FDA-approved to treat any disease. Understanding these differences helps inform tissue banking decisions.
Important Disclaimer: Save My Fat does not provide FDA-approved treatments or cures for any disease. Banking adipose tissue does not guarantee eligibility, access, or clinical benefit from any future therapy, clinical trial, or medical program. All content is for educational purposes only and does not constitute medical advice. Patients must consult their own licensed healthcare professionals regarding all medical decisions.
Maybe a doctor or clinic has told you that one stem cell source is “better” than the other. Maybe you have seen marketing claims that promise results from bone marrow concentrate or fat-derived stem cells. The truth is more nuanced. Each source has distinct biological strengths, and neither is FDA-approved for treating any disease.
This guide compares the two sources side by side using published, peer-reviewed research. You will learn how each source is collected, how the cell yields compare, what researchers have found about their biological behavior, and how the FDA classifies products from each source. By the end, you will have the facts you need to evaluate your options clearly.
Two Tissue Sources, One Cell Type
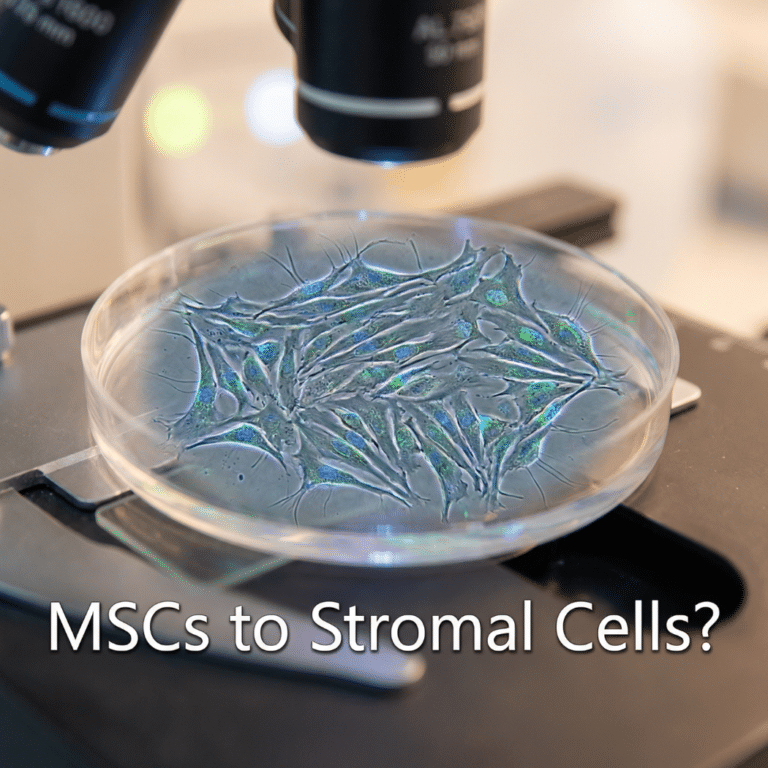
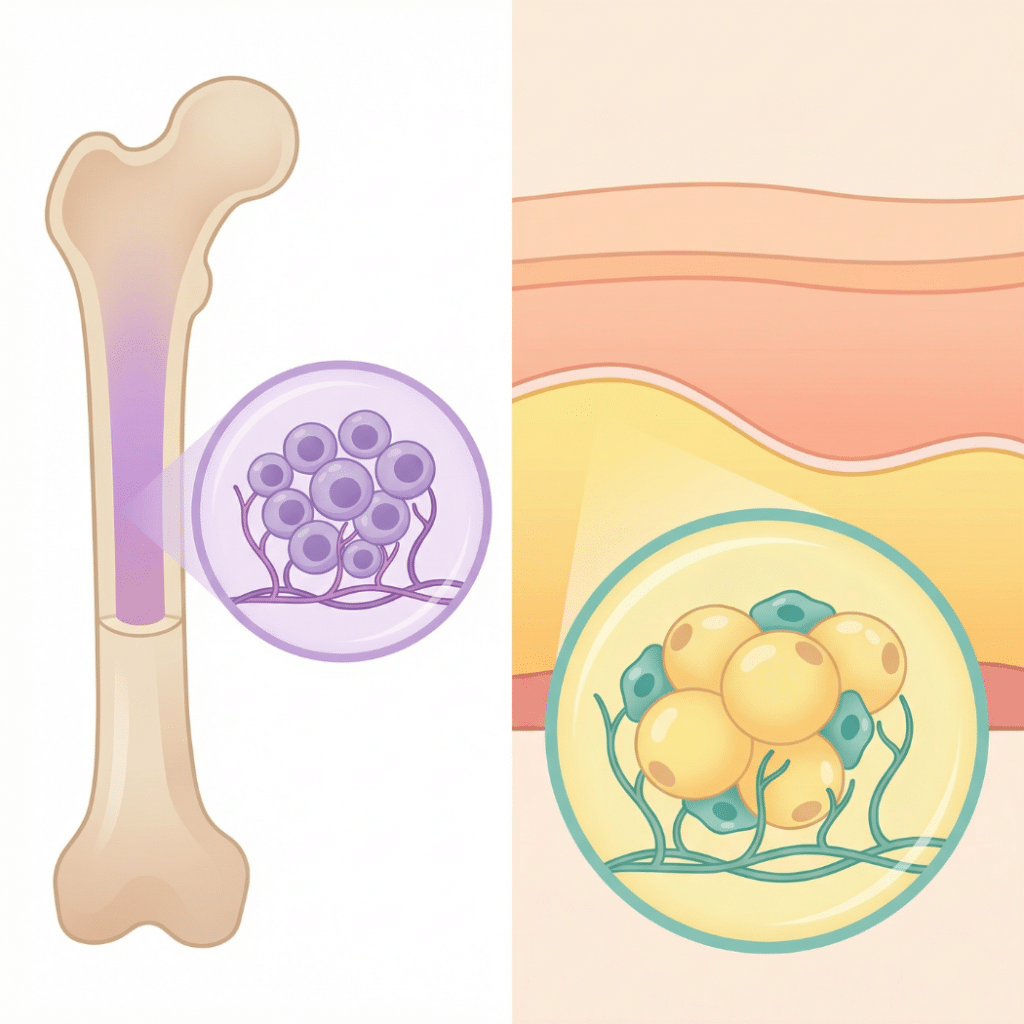
Both bone marrow and adipose tissue contain mesenchymal stem cells (MSCs), a type of adult stem cell that can self-renew and develop into fat, bone, and cartilage cells in lab conditions. For a full introduction to what MSCs are and how they are identified, see the companion guide: What Are Adipose-Derived Stem Cells?
While MSCs from both sources share the same basic classification and meet the same minimum criteria set by the International Society for Cellular Therapy (Bourin et al., 2013), published research has revealed important differences. These include how many stem cells each source yields, how quickly the cells multiply, which cell types they tend to become, and what chemical signals they release (Li et al., 2015).
Understanding these differences matters for anyone considering adipose tissue banking or evaluating stem cell products being marketed by clinics.
How Each Source Is Harvested
The collection process is one of the first practical differences patients notice. Each procedure involves a different part of the body, a different level of invasiveness, and a different recovery experience.
Bone Marrow Aspiration
Bone marrow aspiration involves inserting a large-bore needle into the posterior iliac crest (the back of the hip bone) to withdraw liquid bone marrow. The procedure typically takes 15 to 30 minutes and is performed under local anesthesia, sometimes with sedation.
Published research on patient-reported pain shows that all patients who receive only local anesthesia report some degree of discomfort during aspiration, ranging from a deep pressure sensation to moderate or severe pain. Adding sedation with midazolam significantly reduces reported pain, dropping the rate of pain to about 29% of cases (Patient-reported pain during BMAB, 2022). Recovery involves localized soreness at the aspiration site for several days to weeks.
The overall safety profile of bone marrow aspiration is well-established, with serious adverse events being rare. Hemorrhage is the primary serious complication, though the overall incidence is low (Safety profile of BMAB, 2019).
Adipose Tissue Collection (Mini-Liposuction)
Adipose tissue collection uses a small-volume liposuction procedure to remove fat from the abdomen, flanks, or thighs. It is performed under local anesthesia and typically takes 30 to 60 minutes. Patients commonly report bruising, mild swelling, and soreness after the procedure, with most discomfort resolving within 3 to 7 days (Chu et al., 2019).
Like any medical procedure, adipose tissue collection carries potential risks including infection, bleeding, and bruising. Patients should discuss all risks with a qualified physician. Learn more about what the collection process involves on the how stem cell banking works page.
Harvesting Comparison Table
| Feature | Bone Marrow Aspiration | Adipose Tissue Collection |
|---|---|---|
| Collection site | Posterior iliac crest (hip bone) | Abdomen, flanks, or thighs |
| Anesthesia | Local anesthesia (sedation recommended) | Local anesthesia (tumescent) |
| Procedure duration | 15 to 30 minutes | 30 to 60 minutes |
| Typical discomfort | Deep pressure/aching; moderate-to-severe pain reported without sedation | Bruising, mild swelling, soreness |
| Recovery timeline | Several days to weeks of localized soreness | 3 to 7 days of mild discomfort |
| Typical volume collected | 50 to 100 mL | 50 to 200 mL |
Sources: Patient-reported pain during BMAB, 2022; Chu et al., 2019
Both procedures are performed as outpatient procedures by qualified physicians. Neither is risk-free, and patient experience varies based on individual health status and provider technique.
Cell Yield: How Many Stem Cells Does Each Source Provide?
This is one of the most significant differences between bone marrow and adipose stem cells, and it is well-documented in published research.
Adipose tissue yields approximately 100 to 1,000 times more MSCs per gram than bone marrow. Bone marrow contains roughly 1 MSC per 10,000 to 100,000 nucleated cells. By contrast, the stromal vascular fraction (SVF) from adipose tissue contains approximately 1 MSC per 30 to 1,000 nucleated cells (Gimble et al., 2013; Li et al., 2015).
Estimated MSC Yield Comparison
| Metric | Bone Marrow | Adipose Tissue |
|---|---|---|
| MSC frequency | ~1 per 10,000 to 100,000 nucleated cells | ~1 per 30 to 1,000 nucleated cells |
| Estimated MSCs per mL | ~10,000 to 50,000 | ~300,000 to 570,000 |
| Typical volume collected | 50 to 100 mL | 50 to 200 mL |
| Total estimated MSC yield | ~0.5 to 2 million | ~50 to 200 million |
Sources: Li et al., 2015; Gimble et al., 2013; Bourin et al., 2013
Why Yield Matters
Fewer cells from bone marrow typically means that culture expansion (growing cells in a lab to increase their numbers) is required to reach large quantities. Culture expansion adds time, cost, and regulatory complexity. In the United States, culture-expanded cells generally fall under the FDA’s Section 351 regulatory pathway, which requires clinical trials and FDA approval before marketing for any disease treatment.
This yield difference is one of the reasons researchers and providers in the regenerative medicine space are studying adipose tissue as a stem cell source.
Proliferation and Expansion Capacity
Once cells are collected, how well they grow in the lab also differs between sources.
Published donor-matched studies (meaning the same patient’s bone marrow and fat tissue were compared under identical conditions) show that ADSCs proliferate faster and retain their multipotency (ability to become multiple cell types) through more passages than BMSCs. BMSCs tend to undergo senescence (cellular aging) earlier in culture (Mohamed-Ahmed et al., 2018).
Specifically, ADSCs reached a cumulative population doubling of approximately 17.2 by passage 5, compared to approximately 13.7 for BMSCs in the same study. Population doubling times for ADSCs are approximately 24 to 48 hours, compared to approximately 72 to 96 hours for BMSCs.
This matters for tissue banking because cells that proliferate well may have greater flexibility for potential future research applications. However, faster proliferation alone does not make one source “better” for any specific use. Both sources remain subjects of active scientific investigation.
Differentiation Potential: Where Each Source May Have an Edge
Both ADSCs and BMSCs can develop into three main cell types in the lab: fat cells (adipogenic), bone cells (osteogenic), and cartilage cells (chondrogenic). This is the minimum requirement for MSC classification. However, published research shows they have different strengths.
Published donor-matched research suggests (Mohamed-Ahmed et al., 2018; Kern et al., 2012; Osteogenic comparison, 2014):
- Osteogenic (bone) differentiation: BMSCs generally show stronger bone-forming ability in both lab and animal studies
- Chondrogenic (cartilage) differentiation: BMSCs also tend to demonstrate more robust cartilage formation
- Adipogenic (fat) differentiation: ADSCs show superior fat cell formation, reaching 95% differentiation in approximately two weeks
- Angiogenic (blood vessel) support: ADSCs show enhanced ability to support new blood vessel formation in published studies (Angiogenesis comparison, 2017)
Neither source is universally “better.” Each has biological strengths that researchers are studying for different potential applications. All of this research is investigational, and no MSC-based therapy from either source is FDA-approved for treating any disease.
For more on the areas where researchers are studying ADSCs, visit the emerging research page and the pages on joint and orthopedic research and wellness and healthy aging.
Immunomodulatory Properties
Both ADSCs and BMSCs show the ability to influence the immune system in published lab research. Scientists call this immunomodulation (the ability of cells to change how the immune system responds).
Published research comparing the two sources has found (Li et al., 2015; Immunomodulatory comparison, 2024):
- ADSCs may be more effective at suppressing T-cell proliferation (a measure of immune suppression)
- BMSCs may have advantages in inhibiting natural killer (NK) cell growth
- ADSCs secrete higher levels of certain signaling molecules, including VEGF, bFGF, and IL-6
- BMSCs secrete higher levels of other molecules, including SDF-1
These different signaling profiles, called the secretome (the full set of molecules a cell releases), mean the two cell types may interact with the body differently. Researchers are studying which profile might be more relevant for different research questions (Elman et al., 2014).
This research is preliminary and does not prove that either cell source is safe or effective for treating any condition. No FDA-approved immunomodulatory therapies exist based on ADSCs or BMSCs.
Regulatory Classification: How the FDA Views Each Source
How the FDA regulates a stem cell product depends on how the tissue is processed and what claims are made about its use. Both bone marrow and adipose tissue fall under 21 CFR Part 1271, the FDA’s framework for human cells, tissues, and cellular and tissue-based products (HCT/Ps).
Bone marrow aspirate concentrate (BMAC): When bone marrow is minimally processed (concentrated but not enzymatically digested or culture-expanded) and used for a homologous purpose, it may qualify as a Section 361 HCT/P. However, if BMAC is marketed for systemic effects or disease-modifying claims, the regulatory risk increases significantly.
Adipose tissue: Adipose tissue that undergoes enzymatic digestion to isolate SVF, or culture expansion to isolate ADSCs, is generally classified by the FDA as more than minimally manipulated. This places it under the Section 351 pathway, requiring IND and BLA for marketing. Mechanically processed microfragmented adipose tissue (MFAT) may qualify under 361, depending on the processing method and intended use.
The critical point: neither BMAC nor SVF/ADSCs are FDA-approved to treat any disease. The only FDA-approved stem cell products in the United States are hematopoietic progenitor cells from cord blood, approved for specific blood disorders only. The FDA has issued consumer alerts about unapproved regenerative medicine products from both tissue sources. Patients should always verify FDA approval status before pursuing any product marketed as a stem cell treatment.
What This Means for Tissue Banking
For patients exploring the option of preserving biological material for potential future use, the comparison between these two sources has practical significance.
Save My Fat focuses on adipose tissue preservation for several reasons: the higher cell yield per collection, the less invasive harvesting method, and the abundance of subcutaneous fat in most adults. A single collection can yield enough material for long-term cryopreservation without requiring repeat procedures.
Banked adipose tissue preserves the full cellular composition (including the ADSCs within it) at the patient’s current biological age. Published research shows that adipose tissue can be cryopreserved for years with meaningful viability retention (Chu et al., 2019). First-degree family members may also potentially qualify to use banked cells under certain guidelines. Visit the family page for more information.
Before You Contact Save My Fat: Adipose tissue banking is a preservation service for potential future opportunities, not a treatment or cure for any disease. Outcomes cannot be guaranteed. All medical decisions must be made with a licensed healthcare provider. Banking does not guarantee access to any therapy, clinical trial, or Expanded Access program.
Frequently Asked Questions
Which has more stem cells, bone marrow or fat? Fat tissue yields approximately 100 to 1,000 times more mesenchymal stem cells per gram than bone marrow. This is one of the most well-documented differences between the two sources.
Is bone marrow aspiration painful? Published studies show all patients receiving local anesthesia only report some discomfort during aspiration. Adding sedation reduces pain significantly. Most patients experience localized soreness for several days to weeks afterward.
Can I bank bone marrow the same way I bank fat? Save My Fat specializes in adipose tissue cryopreservation. Bone marrow banking is offered by different types of facilities, typically for hematopoietic (blood-forming) stem cells rather than MSCs. The logistics, cell types preserved, and intended uses differ between the two.
Are bone marrow stem cells better than fat stem cells? Neither source is universally “better.” Published research shows BMSCs may have advantages in bone and cartilage differentiation, while ADSCs may have advantages in yield, proliferation, and certain signaling properties. The best source depends on the research application being studied.
Does the FDA approve either source for disease treatment? No. No MSC-based therapy from bone marrow or adipose tissue is FDA-approved for treating any disease. The only FDA-approved stem cell products are cord blood-derived hematopoietic progenitor cells for specific blood disorders.
Why does Save My Fat focus on adipose tissue instead of bone marrow? Adipose tissue offers practical advantages for banking: significantly higher cell yield, a less invasive collection procedure, and plentiful subcutaneous fat in most adults. Visit the about page for more on the science behind this focus.
Can ADSCs do everything BMSCs can do? Both can differentiate into fat, bone, and cartilage cells. However, published research shows differences in how strongly each source favors certain lineages and how they interact with the immune system. They share the same classification but are not identical in behavior.
How do I decide which source is right for me? Start by understanding what you are trying to accomplish. For patients interested in preserving a rich source of MSCs, adipose tissue offers strong advantages in cell yield and accessibility. For questions about specific medical needs, consult a qualified healthcare provider.
What is BMAC, and is it the same as bone marrow stem cells? BMAC stands for bone marrow aspirate concentrate. It is bone marrow that has been concentrated to increase the proportion of certain cell types, including MSCs. It is not the same as isolated, culture-expanded bone marrow stem cells. BMAC contains a heterogeneous mix of cells.
Are there clinical trials comparing the two sources? Yes. Registered trials on ClinicalTrials.gov include studies comparing bone marrow and adipose-derived MSCs for various research applications (for example, NCT03818737). Listing on ClinicalTrials.gov does not mean a product is proven safe, effective, or FDA-approved.
Key Takeaways
Both Sources Contain MSCs, But They Are Not Identical
- Bone marrow and adipose tissue both provide mesenchymal stem cells
- Published research shows meaningful differences in yield, proliferation, differentiation, and signaling
Fat Tissue Offers a Significant Yield Advantage
- Approximately 100 to 1,000 times more MSCs per gram than bone marrow
- A single collection can yield 50 to 200 million MSCs versus 0.5 to 2 million from bone marrow
Each Source Has Different Biological Strengths
- BMSCs may have edges in bone and cartilage differentiation
- ADSCs may have edges in proliferation, angiogenic support, and certain immunomodulatory functions
Neither Source Is FDA-Approved to Treat Any Disease
- The only approved stem cell products are cord blood-derived cells for blood disorders
- Both BMAC and SVF/ADSCs remain investigational for all other uses
Collection Methods Differ in Invasiveness
- Fat collection uses mini-liposuction under local anesthesia
- Bone marrow requires needle aspiration into the hip bone
Banking Preserves Cells for Potential Future Use
- Adipose tissue banking is a preservation service, not a treatment
- Banking does not guarantee access to any therapy, trial, or clinical benefit
Learn More About Adipose Tissue Banking
For patients and providers interested in understanding how adipose tissue banking works, what the process involves, and what to expect, the next step is to explore the resources on Save My Fat’s website.
Visit the how stem cell banking works page to learn about the preservation process.
For questions about pricing or to connect with a provider, visit the providers page.
Last updated: March 5, 2026