If you are considering adipose tissue banking, or have already scheduled a procedure, one of the most natural questions you can have is: what actually happens to my tissue after it leaves my body? The answer is a carefully sequenced process governed by federal regulations and informed by decades of cryobiology research. This guide walks through every stage from mini-liposuction collection through long-term cryogenic storage, explaining what happens at each step, why it matters for preserving tissue quality, and what quality controls protect your sample along the way.
TLDR: Adipose tissue banking involves six stages: a consultation and eligibility assessment, a minimally invasive mini-liposuction procedure (approximately 30 to 60 minutes, outpatient, local anesthesia), immediate tissue washing and layer separation, addition of a cryoprotective agent, controlled-rate freezing at 1 to 2 degrees Celsius per minute, and long-term vapor-phase liquid nitrogen storage at -150 to -196 degrees Celsius. Published research supports post-thaw viability of 80 to 91 percent with standard protocols, and decade-long storage data shows no significant viability loss compared to fresh tissue. Banking is a preservation service, not a treatment. Read on for the complete step-by-step picture.
Important Disclaimer: Save My Fat does not provide FDA-approved treatments or cures for any disease or medical condition. Adipose tissue banking is a preservation service for potential future opportunities, not a therapeutic product. Banking adipose tissue today does not guarantee eligibility, access, or clinical benefit from any future therapy, clinical trial, or medical program. All content here is for educational and informational purposes only and does not constitute medical advice. Patients must consult their own licensed healthcare professionals regarding all medical decisions. Outcomes of any regenerative medicine research or future therapies are highly individual and cannot be predicted or guaranteed.
The moment your lipoaspirate leaves the procedure room, it begins a journey through a series of steps that have been developed, validated, and refined over years of tissue banking research. Patients who understand that journey tend to feel more confident about their decision, and more prepared to ask the right questions when evaluating banking providers.
Banking adipose tissue is not like dropping off a sample and hoping for the best. Each stage, from the way tumescent anesthesia is formulated to the rate at which your tissue is cooled, reflects specific scientific reasoning. A cooling rate that is even slightly too fast or too slow can meaningfully reduce how many cells survive the process. The temperature at which your tissue is ultimately stored is not arbitrary but is the point at which all biological activity stops, including degradation. These choices are built on published cryobiology data accumulated over decades.
This article walks through all six stages in sequence. By the end, you will understand not just what happens to your tissue but why each step is done the way it is, what would go wrong if it were done differently, and what safeguards are in place to protect your sample throughout its time in storage.
The Six Stages of Adipose Tissue Banking
The banking process moves through six sequential stages, each building on the last. Understanding the full map before diving into each stage makes the details easier to follow.
| Stage | What Happens | Why It Matters |
|---|---|---|
| Consultation | Physician reviews patient history, discusses realistic expectations, confirms candidacy | Ensures appropriate candidates are selected and expectations are calibrated to what banking can and cannot do |
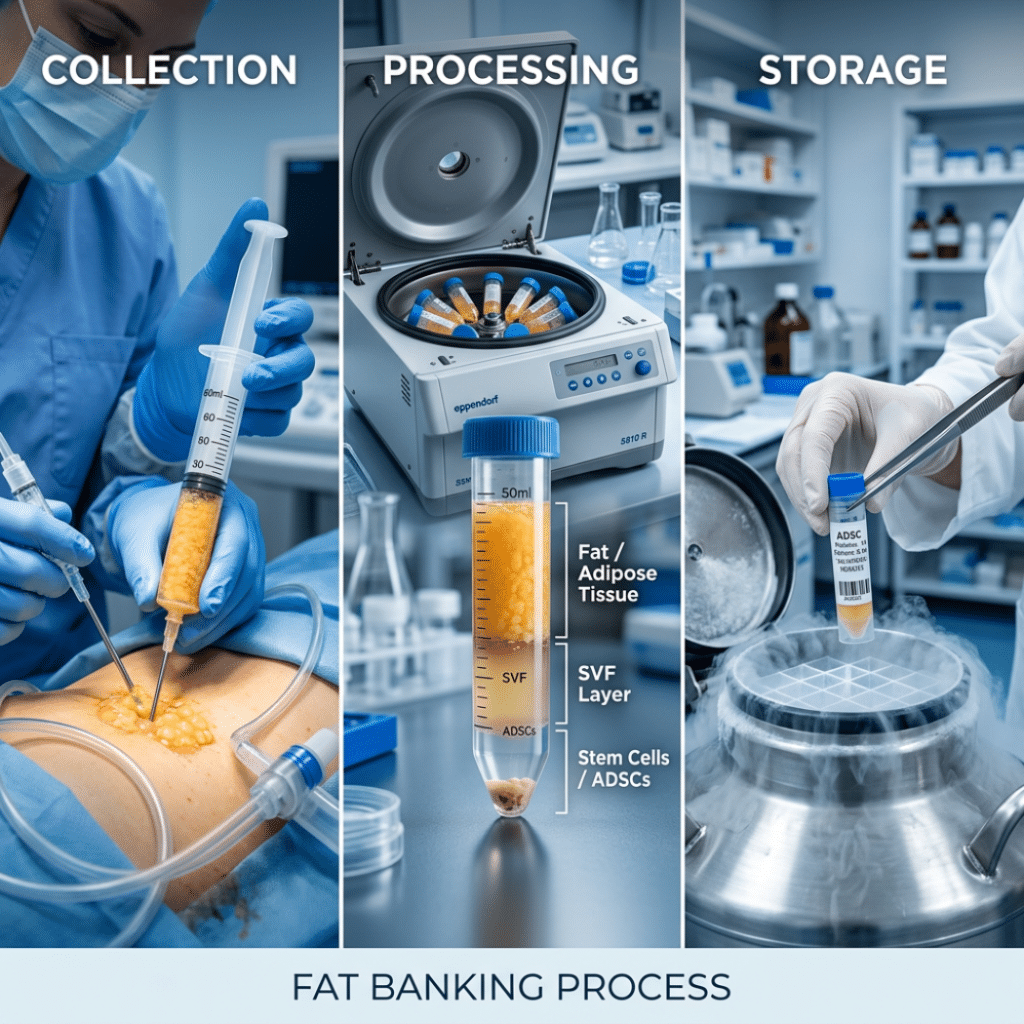
| Collection | Mini-liposuction under local anesthesia, approximately 30 to 60 minutes | Obtains sufficient intact adipose tissue in a way that preserves cell viability |
| Processing | Washing, centrifugation, and layer separation | Removes blood, fluid, and free lipid; isolates the intact adipose tissue layer containing the full cellular ecosystem |
| Cryoprotectant Addition | DMSO-based solution added at cold temperatures | Prevents ice crystal formation that would physically destroy cell membranes during freezing |
| Controlled-Rate Freezing | Temperature drops at 1 to 2 degrees Celsius per minute through the critical zone | Allows water to leave cells safely while minimizing solute-induced dehydration damage |
| Long-Term Storage | Vapor-phase liquid nitrogen at -150 to -196 degrees Celsius | Halts all biological activity and enzymatic degradation; preserves tissue for potential future use |
Stages 1 and 2: Consultation and Collection
What to Expect at the Consultation
The process begins with a physician consultation before any procedure is scheduled. The physician reviews your medical history, discusses what adipose tissue banking is (a preservation service for potential future use in FDA-regulated pathways), and confirms that you are an appropriate candidate for an outpatient procedure under local anesthesia. Informed consent is obtained at this stage. For those still identifying a qualified participating provider, the Save My Fat providers page lists physicians who offer this service.
It bears stating clearly here: the consultation is also where realistic expectations should be established. Banking preserves tissue. It does not provide treatment, enroll anyone in a clinical trial, or guarantee access to any future therapy. A physician who skips this conversation or implies otherwise is a red flag.
The Mini-Liposuction Procedure
The collection itself is a minimally invasive procedure using the tumescent technique, the same foundational approach used in cosmetic liposuction, adapted for smaller volumes. Clinical trial protocols including NCT02869061, registered on ClinicalTrials.gov, document the procedure duration at approximately 30 to 60 minutes with same-day outpatient discharge. Here is exactly what happens:
The harvest site is cleaned and sterilized. The most common locations are the abdomen, flanks, and thighs, all areas with abundant subcutaneous fat and good accessibility. A tumescent solution containing saline, lidocaine (the local anesthetic), and epinephrine (to minimize bleeding) is injected into the subcutaneous fat layer. The solution is allowed to equilibrate for 20 to 30 minutes, during which the tissue swells and the anesthetic takes full effect.
A small blunt-tipped cannula, typically 3 to 4 millimeters in diameter, is inserted through a small incision. Manual or low-pressure powered suction draws out the lipoaspirate. For banking purposes, approximately 100 to 200 milliliters are collected, which is considerably less than cosmetic liposuction procedures that may remove several liters. The incision site is dressed and the procedure is complete. Patients are discharged the same day and typically return to normal activities within 24 to 48 hours.
| Harvest Site | Typical SVF Cell Yield | Practical Notes |
|---|---|---|
| Abdomen | 2 to 5 x 10^5 SVF cells per mL | Most common; abundant tissue availability in most adults |
| Flanks | Similar to abdomen | Good accessibility; commonly used as alternative |
| Thighs | 1.5 to 3 x 10^5 SVF cells per mL | Adequate for banking volumes |
| Infrapatellar fat pad | Lower total volume | Only accessible during knee surgery; higher cell concentration per mL |
Patients should anticipate mild to moderate soreness at the harvest site for 3 to 7 days. Like any medical procedure, mini-liposuction carries potential risks including infection, bleeding, bruising, and adverse reactions to local anesthesia. A complete risk discussion with your physician before the procedure is essential.
Stage 3: Processing and Separation
From the moment the lipoaspirate is collected, time matters. The tissue is transported in a closed, temperature-controlled container to the processing area. Once there, it undergoes a washing and separation protocol designed to isolate the biologically relevant portion of what was collected.
The lipoaspirate is washed with a physiological buffer solution to remove blood, residual tumescent fluid, and free lipid (oil released from fat cells that were ruptured during collection). The washed tissue is then centrifuged at low speed. This separates it into three distinct layers, a separation method referenced in clinical trial protocols including NCT02513238:
The top layer is free lipid oil released from disrupted fat cells. It is discarded. The middle layer is intact adipose tissue, the portion retained for banking. This layer contains the full cellular ecosystem: adipose-derived mesenchymal stromal cells (ADSCs), other stromal vascular fraction (SVF) cells, the supporting extracellular matrix, and associated blood vessel components. The bottom layer is an aqueous layer containing blood, tumescent fluid remnants, and cellular debris. It is discarded.
Only the middle layer proceeds to the next stage.
Why Intact Tissue Banking Differs from SVF Processing
This is one of the most important regulatory distinctions in the adipose tissue banking space, and it is worth understanding precisely. The FDA’s November 2017 guidance on minimal manipulation and homologous use (available at fda.gov/media/109176/download) addresses how adipose tissue products are classified. The FDA's HCTP framework and 21 CFR Part 1271 govern these determinations.
Washing and centrifugation to separate intact adipose tissue layers is processing that may qualify as minimal manipulation under these regulations. By contrast, enzymatic digestion, using collagenase to break down adipose tissue and release SVF cells, is classified by the FDA as more than minimally manipulated. The 2024 Ninth Circuit Court ruling further confirmed that enzymatically processed SVF constitutes a drug under the Federal Food, Drug, and Cosmetic Act. That classification places it under Section 351 of the Public Health Service Act, requiring an Investigational New Drug application and ultimately a Biologics License Application before any such product can be legally marketed for treating disease.
| Processing Method | What It Produces | FDA Classification | Regulatory Pathway |
|---|---|---|---|
| Washing and centrifugation only | Intact adipose tissue with full cellular ecosystem | Potentially minimally manipulated structural tissue | Section 361 HCTP if all four regulatory criteria are met |
| Enzymatic digestion (collagenase) | Stromal vascular fraction, heterogeneous cell mixture | More than minimally manipulated | Section 351, requires IND or BLA |
| Culture expansion | Pure ADSC population | More than minimally manipulated | Section 351, requires IND or BLA |
Save My Fat banks intact adipose tissue. SVF isolation or ADSC culture expansion can occur later, if and when a patient enters an FDA-regulated clinical pathway that requires processed cells. That future processing would occur under the appropriate regulatory oversight applicable to the specific pathway at that time, not as part of the banking service itself. For more context on the biology of these cells and why researchers study them, the patient’s guide to adipose-derived stem cells covers that science in detail.
Stage 4: Cryoprotectant Addition
Why Unprotected Freezing Destroys Cells
To understand why cryoprotective agents are necessary, it helps to understand what happens without them. When biological tissue freezes without protection, water inside and around cells begins to crystallize. Intracellular ice crystals grow sharp edges that physically puncture cell membranes from the inside. Extracellular ice compresses the cells from outside. The simultaneous osmotic stress from solutes concentrating outside the cell as water freezes pulls remaining intracellular water outward, causing dehydration. The compound result is widespread, irreversible cell death. This is also the same process that makes frozen vegetables mushy when thawed: the ice crystals that form in unprotected plant cells rupture cell walls, destroying structure.
| Factor | Unprotected Freezing | Cryopreservation with CPA |
|---|---|---|
| Ice crystal formation | Large intracellular crystals form and puncture membranes | Minimized by cryoprotective agents and controlled cooling rate |
| Cell membrane integrity | Frequently ruptured | Largely preserved |
| Osmotic stress | Severe and uncontrolled | Managed through CPA concentration and gradual addition |
| Post-thaw viability | Very low; most cells destroyed | 80 to 91 percent in published research (Thirumala et al., 2010) |
| Preserved function | Severely compromised | Cells retain phenotype, proliferation capacity, and differentiation potential |
How Cryoprotective Agents Work
The standard cryoprotective agent (CPA) for adipose tissue banking is dimethyl sulfoxide (DMSO), typically used at a concentration of 10 percent. DMSO is a small molecule that permeates cell membranes relatively easily. Once inside the cell, it partially displaces intracellular water and lowers the freezing point of the cell’s interior. This reduces the size and formation rate of ice crystals that would otherwise cause membrane damage. Published research by Thirumala and colleagues in 2010 established that DMSO concentrations between 5 and 10 percent show no significant differences in ADSC viability, and documented post-thaw viability of 80 to 91 percent using standard protocols.
DMSO is added gradually at or below 4 degrees Celsius, specifically because CPA addition at warmer temperatures creates osmotic shock that itself causes cell death. The gradual cold-temperature addition allows cells to equilibrate to the new osmotic environment before freezing begins. DMSO must be removed through washing steps before any future clinical application, as it can cause cell toxicity with prolonged exposure at body temperature.
Researchers are also investigating alternatives to DMSO, including trehalose (a non-toxic disaccharide sugar), L-proline combined with trehalose, and chemically defined xeno-free formulations. A 2023 study by Zanata and colleagues found that L-proline combined with trehalose produced viability equivalent to DMSO after 90 days of storage at -80 degrees Celsius, which is a meaningful finding for patients or facilities seeking non-toxic alternatives. These alternatives are promising, though DMSO-based protocols currently remain the standard with the most extensive long-term published data.
Stage 5: Controlled-Rate Freezing and Long-Term Storage
Why the Cooling Rate Matters
This is arguably the stage where the most damage can occur if done incorrectly. The physics of ice formation during cooling create a narrow window in which cells are at maximum risk, and the cooling rate determines whether cells pass through that window safely or not.
Cooling too fast causes intracellular ice formation: water does not have time to leave the cell before it freezes, and ice nucleates inside the membrane where it causes the most damage. Cooling too slowly causes a different problem: prolonged exposure to the increasingly concentrated solutes outside the cell (as the external water freezes out first) pulls water out of the cell through osmosis, causing severe dehydration. Published cryobiology research by Shu and colleagues in 2015 confirmed that the optimal cooling rate for ADSCs is 1 to 2 degrees Celsius per minute. A 2025 systematic review by Bonomi and colleagues confirmed this as the most commonly applied protocol across the literature, with encouraging outcomes for tissue survival and histological structure preservation.
Achieving this rate requires either a programmable controlled-rate freezer, which uses a computer to precisely modulate liquid nitrogen injection to maintain the target cooling slope, or a validated isopropanol-based passive cooling container that achieves the same rate through passive thermal conduction. The tissue passes through the critical zone between -15 and -60 degrees Celsius at the controlled rate, where ice nucleation risk is highest. Once through this zone, the tissue reaches -80 degrees Celsius as an intermediate step before transfer to long-term liquid nitrogen storage.
Long-Term Storage at Liquid Nitrogen Temperatures
At -196 degrees Celsius (direct liquid nitrogen contact) or -150 to -180 degrees Celsius (vapor phase), all enzymatic reactions stop completely. All metabolic activity ceases. There is no ongoing chemical degradation. The tissue is, in the most literal biological sense, paused.
Vapor-phase storage is the preferred method for clinical-grade tissue because it eliminates the risk of cross-contamination between samples that can occur in liquid-phase storage, while maintaining temperatures well below the biological activity threshold. The vapor above liquid nitrogen in a properly maintained cryotank stays between -140 and -180 degrees Celsius, which is more than sufficient to halt all biological processes.
| Storage Temperature | Method | Biological Activity | Practical Duration | Published Viability Notes |
|---|---|---|---|---|
| 4 degrees C | Refrigerator | Active, slow degradation | Hours to days | Near-fresh; short-term only |
| -80 degrees C | Ultra-low freezer | Greatly reduced | 12 to 18 months | Approximately 80 percent at 9 months |
| -150 degrees C | Vapor-phase nitrogen | Effectively halted | 18 months and beyond | 85 percent at 18 months; 90 percent at 24 months in cryobag format |
| -196 degrees C | Liquid nitrogen | Completely halted | Theoretically indefinite | 90-plus percent at 24 months; decade-long data shows no significant difference from fresh tissue (Tsekouras et al., 2018) |
Quality Controls That Protect Your Sample
Viability is validated before the tissue goes into long-term storage. Pre-freeze viability testing establishes a documented baseline for each individual sample. Sterility testing through microbiological cultures confirms the absence of contamination before cryopreservation. Cell count and characterization document the cellular content of the stored material. Continuous temperature monitoring with automated alarm systems ensures that any equipment deviation triggers an immediate response before tissue is compromised. Chain of custody documentation tracks every sample from collection through storage, and unique patient identifiers on all containers prevent any possibility of mix-up.
These quality control measures are not optional features. Banking facilities operating as human cells, tissues, and cellular and tissue-based products (HCT/P) establishments are required to register with the FDA and comply with current good tissue practice (cGTP) regulations under 21 CFR Part 1271. When evaluating any banking provider, asking specifically about their CGTP compliance status, their temperature monitoring infrastructure, and their backup protocols is not overcaution. It is the appropriate due diligence.
Stage 6: Retrieval and Thawing
When banked tissue is requested for use in an FDA-regulated clinical pathway, whether a clinical trial, an Expanded Access program, or a future approved therapy, the retrieval process begins with identity verification and chain of custody confirmation. Patient identity and consent for retrieval are verified before any sample is moved.
The tissue is thawed using a rapid thawing protocol in a 37-degree Celsius water bath. Counterintuitively, rapid thawing (typically 1 to 2 minutes) is better for cell survival than slow thawing. Slow warming through the critical temperature zone allows small ice crystals that formed during cooling to grow larger through a process called recrystallization, causing additional mechanical damage. Rapid thawing passes through this zone before significant recrystallization can occur.
After thawing, DMSO is removed through serial dilution washing steps before any clinical use. Post-thaw viability assessment confirms that the sample meets quality benchmarks before it is released. Because tissue is typically stored in multiple separate cryovials rather than a single container, individual vials can be thawed for a specific purpose while the remaining vials stay undisturbed in cryogenic storage.
Retrieval occurs only for use in an FDA-regulated clinical pathway. The patient or their authorized representative must provide consent for retrieval. Any future clinical use of retrieved tissue must comply with applicable FDA regulations at that time. For context on what those regulated pathways look like, the guide to Expanded Access programs describes the compassionate use framework in plain language. The overview of what adipose tissue banking involves and preserves covers the broader context of why banking may be relevant to future FDA-regulated opportunities.
What the Published Viability Data Shows
Published cryobiology research provides specific, peer-reviewed data on what to expect from properly banked adipose tissue. The table below summarizes the key findings.
| Study | Storage Duration | Storage Conditions | CPA Used | Post-Thaw Viability | Key Finding |
|---|---|---|---|---|---|
| Thirumala et al., 2010 | 3 months | -196 degrees C | 10% DMSO | 80 to 91 percent | Standard protocol benchmark established |
| Miyagi-Shiohira et al., 2021 | 18 months | -150 degrees C | DMSO/CP-1 | 85 percent | High-density vapor-phase storage validated |
| Miyagi-Shiohira et al., 2021 | 24 months | -150 degrees C | DMSO | 90 percent (cryobag format) | Large-scale storage confirmed feasible |
| Tsekouras et al., 2018 | Over 10 years | Liquid nitrogen | DMSO-based | No significant difference from fresh | Immunophenotype, proliferation, and differentiation preserved after a decade |
| Zanata et al., 2023 | 90 days | -80 degrees C | L-proline and trehalose | Equivalent to DMSO | Non-toxic alternative validated for short-term |
| Devitt et al., 2015 | Up to 1,159 days | Cryogenic | Standard | Viable cells isolated successfully | Patient age (8 to 82 years) did not impact outcomes |
| Gonda et al., 2019 | Long-term biobank | Intact lipoaspirate | Standard | 67 percent volume recovery average | No relationship between recovery and patient age |
High post-thaw viability means the cells survived the freeze-thaw cycle with their basic biological properties intact. It does not guarantee that banked tissue will qualify for any specific clinical trial, produce any specific clinical outcome, or be compatible with any future therapeutic application. Those determinations depend on regulatory, clinical, and scientific factors that are entirely separate from the storage process itself. No adipose-derived stem cell product is FDA-approved to treat any disease as of April 2026.
Frequently Asked Questions
How long does the mini-liposuction collection procedure take?
The procedure itself takes approximately 30 to 60 minutes, consistent with protocols documented in ClinicalTrials.gov registrations for adipose tissue collection studies. Including preparation time, tumescent fluid equilibration, and post-procedure observation, patients should plan for a total clinic visit of 2 to 3 hours. Patients are typically discharged the same day with written aftercare instructions.
Is the collection procedure painful?
Tumescent local anesthesia is designed to make the procedure comfortable during the collection itself. Patients typically feel pressure, movement, or mild tugging but should not experience sharp pain during the procedure. Mild to moderate soreness at the harvest site is common for 3 to 7 days after the procedure. Like any procedure involving incisions and anesthesia, mini-liposuction carries potential risks including infection, bleeding, bruising, and adverse reactions. A thorough risk discussion with your physician before proceeding is essential.
How much fat is collected?
A banking collection typically involves approximately 100 to 200 milliliters of lipoaspirate, considerably less than the several liters that may be removed in cosmetic liposuction. The amount collected is calibrated to provide sufficient intact tissue for banking without requiring an unnecessarily large procedure.
Why is my tissue stored as intact fat rather than isolated stem cells?
Banking intact adipose tissue, without enzymatic digestion, may qualify as minimal manipulation under FDA regulations (21 CFR Part 1271), which carries significantly less regulatory burden than processing to isolate SVF or culture-expand ADSCs. Both SVF isolation via enzymatic digestion and culture expansion place the product under Section 351, requiring IND applications and FDA approval before clinical use. Banking intact tissue first preserves the cellular ecosystem in its most regulatory-favorable state. If a future FDA-regulated pathway requires processed cells, that isolation can occur under the regulatory framework appropriate to that pathway at that time.
What is DMSO and is it safe?
DMSO (dimethyl sulfoxide) is the most widely studied cryoprotective agent in stem cell and tissue banking, with decades of use in cord blood, bone marrow, and now adipose tissue preservation. At concentrations of 5 to 10 percent, it is effective and well-characterized. It can be toxic at higher concentrations or with prolonged exposure at physiological temperatures, which is why protocols add it gradually at cold temperatures and why it must be removed by washing before any future clinical application.
What happens if the storage facility has a power failure or equipment problem?
Compliant tissue banking facilities maintain continuous temperature monitoring with automated alarms, redundant liquid nitrogen supply systems, and documented emergency response procedures. These safeguards are infrastructure requirements for facilities operating under CGTP compliance (21 CFR Part 1271). Before banking with any facility, ask specifically about their monitoring systems, backup nitrogen supply, and documented emergency protocols.
Does my age affect how well my tissue can be stored?
Published research by Devitt and colleagues in 2015 successfully isolated viable ADSCs from tissue cryopreserved across donor ages ranging from 8 to 82 years, with patient age not found to significantly impact isolation success, viability, or proliferative outcomes. Research by Gonda and colleagues in 2019 similarly found no relationship between patient age and post-thaw tissue volume recovery. That said, cells collected at a younger biological age may have different properties than cells collected later in life, which is one reason many patients choose to bank sooner rather than waiting.
Can I have my tissue thawed in stages rather than all at once?
Yes. Tissue is divided into multiple individually labeled cryovials before freezing. Each vial can be thawed independently as needed for a specific authorized purpose while the remaining vials stay undisturbed in long-term storage. This design is standard in tissue banking for exactly this reason.
Key Takeaways
The process is defined, regulated, and sequential. Six stages from consultation through long-term storage, each governed by federal regulations under 21 CFR Part 1271 and informed by validated cryobiology research.
Collection is minimally invasive and outpatient. Mini-liposuction under local anesthesia takes approximately 30 to 60 minutes. Most patients return to normal activities within 24 to 48 hours, though the procedure carries real medical risks that require full discussion with a physician.
Intact tissue banking has specific regulatory significance. Avoiding enzymatic digestion preserves the full cellular ecosystem and may qualify the product as minimally manipulated under FDA regulations, keeping future processing options open under appropriate regulatory oversight.
Cryoprotection and controlled cooling are not optional steps. DMSO prevents ice crystal destruction of cells. The 1 to 2 degrees Celsius per minute cooling rate is scientifically validated to minimize cell death during the freeze. Unprotected or poorly controlled freezing destroys cells irreversibly.
Liquid nitrogen temperatures halt all biological activity. Storage at -150 to -196 degrees Celsius is not simply a cold freezer. It is suspended animation for living tissue. All metabolic processes stop, and degradation does not occur.
Published data supports long-term viability. Post-thaw viability of 80 to 91 percent with standard protocols, and decade-long storage data showing no significant difference from fresh tissue (Tsekouras et al., 2018), give the banking process an evidence base that goes beyond manufacturer claims.
Quality controls are integrated at every stage. Pre-freeze viability testing, sterility confirmation, chain of custody documentation, and continuous temperature monitoring are requirements, not optional services.
Banking is preservation, not treatment. No ADSC product holds FDA approval for any disease as of April 2026. Banking preserves a biological option for a future whose regulatory and scientific landscape continues to evolve. For context on what that landscape looks like and where research is heading, the emerging research section provides an ongoing overview.
Medical and Regulatory Disclaimer
Save My Fat does not provide FDA-approved treatments or cures for any disease or medical condition. Nothing in this article describes, promotes, or constitutes a treatment, therapy, or medical intervention of any kind. Adipose tissue banking is a tissue preservation service for potential future opportunities that may arise as regenerative medicine science and FDA regulations evolve. It is not a therapeutic product and does not provide clinical benefit.
Banking adipose tissue today does not guarantee eligibility, access, or clinical benefit from any future therapy, clinical trial, Expanded Access program, or Right to Try pathway. Any future use of banked tissue depends entirely on the regulatory status of products or procedures at that time, the patient’s clinical situation and physician guidance, and the availability of FDA-regulated pathways that may accept previously banked autologous material.
All content in this article is for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment recommendations. Patients must consult their own licensed healthcare professionals regarding all decisions related to their health, medical care, and participation in any research program.
Learn More
For more context on the cells this process preserves and why researchers study them, the patient’s guide to adipose-derived stem cells explains the biology in plain language. For a complete overview of what banking involves from a patient’s perspective, the complete guide to adipose tissue banking covers the full picture. For a concise step-by-step overview of how stem cell banking works, that resource walks through the process in a more condensed format. For patients interested in the regulatory pathways through which banked tissue might eventually be used, the guide to Expanded Access programs covers the compassionate use framework, and the For Patients section provides a starting point for the broader conversation.
This article is for educational purposes only and does not constitute medical advice. Legal and medical review is required before publication. Please consult your licensed healthcare provider regarding all medical decisions.
Last Updated: April 8, 2026