If you’re curious about what actually happens when adipose tissue is preserved for long-term storage, you’re asking the right question. Understanding the science behind cryopreservation helps you evaluate whether tissue banking aligns with your health planning goals. This guide walks you through the validated protocols, equipment, and quality control measures that make long-term tissue preservation possible, giving you the clarity to make informed decisions.
TLDR: Adipose tissue cryopreservation uses validated scientific protocols to preserve tissue at ultra-low temperatures for potential future use. The process involves careful preparation, cryoprotectant solutions, controlled-rate freezing, and liquid nitrogen storage. Post-thaw viability rates of 80-91% have been documented in peer-reviewed studies. Understanding this process helps you ask the right questions when evaluating tissue banking services.
Important Note: Save My Fat does not provide FDA-approved treatments or cures. Cryopreservation is a preservation service for potential future opportunities, not a therapeutic product. Understanding the cryopreservation process does not guarantee eligibility, access, or clinical benefit from any future therapy. All content is for educational purposes only and does not constitute medical advice. Patients must consult their own licensed healthcare professionals regarding all medical decisions.
You’ve probably heard terms like “cryopreservation” and “tissue banking” but wondered what actually happens at the molecular level when tissue is frozen for years or even decades. It’s a fair question. Unlike dropping leftovers in your home freezer, preserving living tissue requires precise control over temperature, timing, and chemistry to keep cells viable.
The stakes matter here. If you’re considering banking your adipose tissue for potential future opportunities, you deserve to understand the science that makes long-term storage possible. Transparent, validated protocols separate compliant tissue banking services from questionable alternatives. When you understand the “how,” you can better evaluate the “whether.”
This guide explains the cryopreservation process step by step, from tissue collection through long-term storage and eventual thawing. You’ll learn why simple freezing damages cells, how cryoprotectants solve this problem, what temperatures are required, and how quality control measures verify success. By the end, you’ll have the scientific foundation to ask informed questions about any tissue banking service you consider.
Why Freezing Living Tissue Is Complex
Freezing tissue isn’t like making ice cubes. Living cells contain water, and when water freezes, it forms ice crystals. These crystals are jagged structures that puncture cell membranes and destroy internal organelles. The result is cell death, rendering the tissue unusable.
The cooling rate creates a biological dilemma. Freeze too quickly, and ice crystals form inside cells before water can escape. Freeze too slowly, and cells lose too much water through osmosis, causing severe dehydration and structural collapse. Either extreme kills cells.
This challenge drove decades of cryobiology research. Scientists needed methods to preserve cells in a state where metabolic activity essentially stops, but cellular structures remain intact. The solution involves two key innovations: cryoprotectant chemicals and precisely controlled freezing rates. Together, these allow tissue to enter a reversible suspended state rather than suffering irreversible damage.
Understanding this fundamental challenge helps explain why validated protocols matter. Every step in the cryopreservation process addresses a specific biological problem. Shortcuts or variations from proven methods can mean the difference between viable tissue and worthless biological material.
What Is Cryopreservation?
Cryopreservation is the process of preserving biological material at sub-zero temperatures while maintaining viability for future use. Unlike simple freezing, cryopreservation uses specialized techniques to prevent ice crystal damage and preserve cellular function.
The principle is straightforward: at extremely low temperatures, metabolic activity slows to near zero. Chemical reactions that cause aging and degradation essentially stop. Cells enter a state of suspended animation where they remain alive but inactive. When properly executed, this state is reversible, meaning tissue can be thawed and cells resume normal function.
Cryopreservation has been used successfully since the 1960s for various biological materials. Reproductive cells, blood products, and tissue samples have been preserved for decades using these principles. The National Institutes of Health has documented extensive research validating cryopreservation methodology across multiple tissue types.
For adipose tissue specifically, peer-reviewed studies have demonstrated successful preservation for 44 months or longer with maintained cell viability. The theoretical storage duration at liquid nitrogen temperatures extends indefinitely, as no measurable degradation occurs at these temperatures. However, practical considerations like facility maintenance and quality monitoring remain important factors in any tissue banking process.
Understanding Cryoprotectants and DMSO
Cryoprotectants are the chemical key to successful tissue preservation. The most commonly used cryoprotectant is dimethyl sulfoxide, known as DMSO. This small organic molecule serves as a cellular antifreeze, preventing the ice crystal formation that would otherwise destroy cells.
DMSO works through several mechanisms. First, it penetrates cell membranes and partially replaces intracellular water. This reduces the amount of water available to form damaging ice crystals. Second, DMSO lowers the freezing point of the remaining solution through what scientists call colligative effects. Third, it helps stabilize cell membranes during the temperature transitions of freezing and thawing.
Standard protocols use 10% DMSO concentration, typically combined with 90% serum or human serum albumin as a base solution. Some emerging protocols use lower DMSO concentrations (5%) combined with trehalose, a sugar that provides additional cryoprotection. The FDA recognizes DMSO for certain medical applications, and at proper concentrations, toxicity risk is minimal.
One important consideration: DMSO can be mildly toxic to cells at room temperature. This means the cryoprotectant must be added when tissue is cold (around 4°C), and exposure time at warmer temperatures must be minimized. During thawing, DMSO is gradually removed through careful washing steps before any potential future use. These handling requirements underscore why validated protocols and trained personnel matter in tissue banking.
| Cryoprotectant | Typical Concentration | Mechanism | Considerations |
|---|---|---|---|
| DMSO | 10% | Membrane penetration, ice prevention | Mild toxicity at room temperature |
| DMSO + Trehalose | 5% + 5% | Combined protection | Emerging protocol |
| Human Serum Albumin | 90% (base) | Cell membrane stability | Carrier solution |
Step-by-Step Cryopreservation Protocol
The cryopreservation process follows a precise sequence designed to maximize cell survival at each stage. Understanding these steps helps you evaluate whether a tissue banking service follows validated methodology.
Step 1: Tissue Collection and Initial Preparation
Adipose tissue is collected via liposuction, typically obtaining 100-200 mL of tissue. The material is transferred to a sterile collection vessel containing antibiotic solution to prevent contamination. Initial processing must occur within two hours of collection to maintain tissue quality.
Basic centrifugation removes excess fluid, including blood and the tumescent solution used during collection. This step concentrates the tissue and removes components that could interfere with cryopreservation.
Step 2: Processing for Cryopreservation
The tissue undergoes washing with sterile saline solution to remove remaining blood, anesthetic, and other contaminants. Centrifugation at 400 RCF (relative centrifugal force) for four to five minutes further removes excess fluid.
Quality assessment occurs at this stage. Technicians evaluate tissue for volume, visible contamination, and overall quality. Any samples that don’t meet standards are flagged for review. This quality gate helps ensure only appropriate material proceeds to freezing.
Step 3: Cryoprotectant Addition
The DMSO solution (typically 10% DMSO in serum or albumin base) is prepared and chilled to 4°C. Tissue and cryoprotectant are combined gradually at cold temperatures, not shocked together at room temperature.
Gradual mixing allows the cryoprotectant to penetrate tissue without causing osmotic damage. An incubation period of 30-60 minutes at cold temperature ensures adequate penetration before freezing begins.
Step 4: Controlled-Rate Freezing
This step is critical for cell survival. The optimal freezing rate is negative one degree Celsius per minute. Faster rates cause intracellular ice formation. Slower rates cause excessive dehydration.
Specialized equipment maintains this precise rate. Programmable controlled-rate freezers or validated passive devices (using isopropanol-based chambers) lower the temperature from 4°C to negative 80°C over approximately 90 minutes.
At negative 80°C, tissue is transferred to liquid nitrogen storage at negative 196°C. This transition must occur promptly to prevent temperature fluctuation.
Step 5: Long-Term Storage
Two storage options exist for cryopreserved tissue:
Short-term storage at negative 80°C (mechanical freezers) is suitable for months but not optimal for years. Long-term storage uses liquid nitrogen, either in vapor phase (negative 140°C to negative 180°C) or liquid phase (negative 196°C).
Liquid nitrogen storage provides indefinite stability because no measurable degradation occurs at these temperatures. Research published in peer-reviewed journals has documented successful tissue recovery after 44 months or longer of cryopreservation.
| Step | Temperature | Duration | Purpose |
|---|---|---|---|
| Collection and Prep | 4°C | 30 minutes | Remove fluid, assess quality |
| DMSO Addition | 4°C | 30-60 minutes | Cryoprotectant penetration |
| Controlled Freezing | 4°C to -80°C | 90 minutes | Prevent ice crystal formation |
| Transfer to LN | -80°C to -196°C | 15 minutes | Begin long-term storage |
| Storage | -196°C | Years to decades | Indefinite viability maintenance |
Quality Control and Monitoring
Quality control distinguishes compliant tissue banking from unregulated operations. Multiple systems work together to verify preservation success and maintain tissue integrity over time.
During Storage
Temperature monitoring occurs continuously using automated sensor systems. Alarms alert staff to any deviation from acceptable ranges. Redundant storage systems, including backup generators and secondary freezers, protect against equipment failure.
Facility inspections and validations occur regularly. Documentation of temperature logs, maintenance records, and any deviations provides traceability required by FDA Current Good Tissue Practice (CGTP) regulations under 21 CFR 1271. Disaster recovery planning addresses scenarios like power failures or natural disasters.
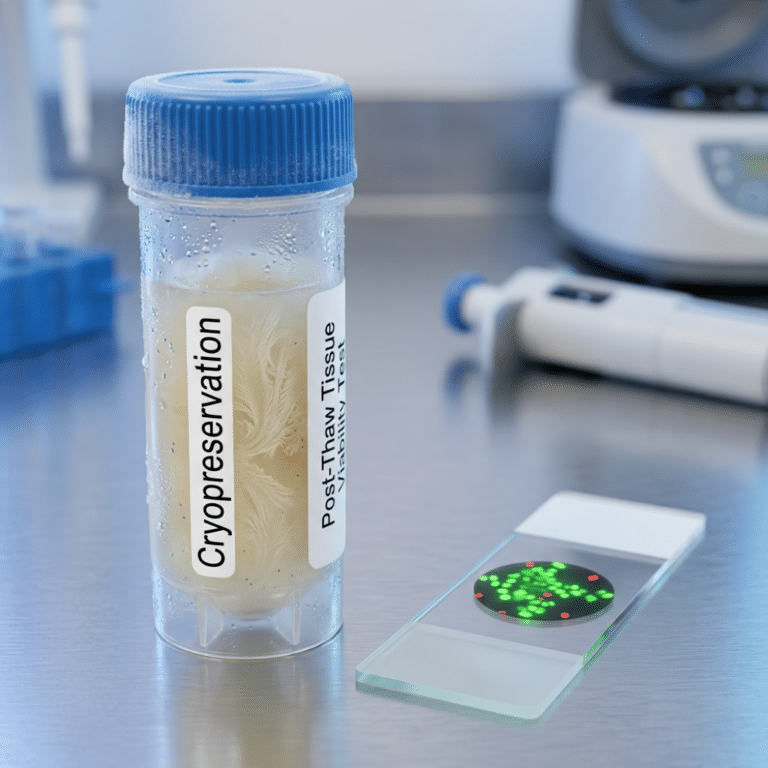
Viability Testing
Quality control may include thawing a small sample (aliquot) from a patient’s tissue to assess post-thaw viability. Testing methods include trypan blue exclusion and flow cytometry, which measure what percentage of cells survive the freeze-thaw cycle.
Typical viability results show 80-91% of cells surviving the thaw process, as documented in multiple peer-reviewed studies. However, it’s essential to understand that viability testing measures technical success of the preservation process. It does not predict or guarantee future therapeutic benefit, clinical trial eligibility, or any specific medical outcome.
Quality Standards
Compliant facilities adhere to established standards including Good Manufacturing Practice (GMP) requirements and Current Good Tissue Practice (CGTP) regulations. Testing includes sterility verification (bacterial, fungal, mycoplasma), endotoxin testing (standard: less than 5 EU/mL), and complete documentation maintaining chain of custody.
| Test | Purpose | Standard | Frequency |
|---|---|---|---|
| Temperature Monitoring | Verify protocol adherence | -1°C/minute freezing rate | Continuous |
| Viability Assessment | Confirm cell survival post-thaw | 70-80% minimum | Pre-banking sample |
| Sterility Testing | Detect contamination | No growth at 14 days | After processing |
| Endotoxin Testing | Safety verification | Less than 5 EU/mL | After processing |
| Donor Screening | Infectious disease exclusion | Negative panel | Before banking |
Safe Thawing and Tissue Recovery
The thawing process is equally important as freezing. Improper thawing can destroy cells that survived cryopreservation perfectly.
Tissue is removed from liquid nitrogen storage and briefly equilibrated at negative 80°C. Controlled warming occurs in a 37°C water bath over 5-10 minutes. The rate matters: warming too rapidly can cause thermal shock, while warming too slowly allows damaging ice recrystallization.
After thawing, DMSO must be removed to prevent cellular toxicity. This occurs through gradual dilution with isotonic saline solutions. Multiple wash cycles prevent osmotic shock that could damage cells recovering from cryopreservation.
Post-thaw assessment verifies success. Visual inspection confirms tissue maintains gross structure, appropriate color, and consistency. If future clinical use is planned through a legitimate pathway, cell count and viability assessment would be performed at that time.
What Could Go Wrong
Transparency about potential problems helps set realistic expectations:
Improper freezing rate causes ice crystal formation and cell death. Temperature fluctuations during storage reduce viability over time. Contamination (bacterial or fungal growth) can compromise samples. Improper thawing causes osmotic shock and cell damage.
These risks are mitigated through validated protocols, trained personnel, quality control systems, and equipment redundancy. Compliant tissue banking services openly discuss their protocols and quality measures. This transparency is a hallmark of legitimate operations and something you should expect from any provider you consider, as outlined on the Save My Fat about page.
Frequently Asked Questions
Q: If viability is 80-91% after thawing, does that mean 80-91% of my tissue survives?
A: Viability and volume retention are different metrics. Volume retention typically ranges from 67-71% in documented studies. Viability measures what percentage of cells within that retained volume are alive and functional. Both measurements matter, but they describe different aspects of preservation success. Neither metric predicts or guarantees any future therapeutic outcome.
Q: Is DMSO toxic to cells?
A: DMSO is necessary for successful cryopreservation, and toxicity risk is minimal at proper concentrations and cold temperatures. DMSO becomes mildly toxic at room temperature with extended exposure, which is why protocols specify cold handling and limited exposure times. Before any potential future use, DMSO is completely removed through washing procedures. The FDA has evaluated DMSO for certain medical applications.
Q: How do you ensure the freezing rate is exactly negative one degree per minute?
A: Programmable controlled-rate freezers contain temperature sensors and computer controls that maintain precise cooling curves. These devices are validated against established protocols and regularly calibrated. Alternative passive devices using isopropanol chambers have been validated to achieve similar rates. Quality control documentation records actual cooling curves for each batch.
Q: What happens if there’s a power outage and tissue thaws?
A: Liquid nitrogen storage doesn’t require electricity. The liquid nitrogen itself maintains temperature, and properly insulated dewars can maintain safe temperatures for days even without refilling. Mechanical freezers (negative 80°C) do require power, which is why facilities use backup generators, alarm systems, and redundant storage locations. Multiple safeguards protect against any single point of failure.
Q: Can tissue be frozen and thawed multiple times?
A: No. Repeated freeze-thaw cycles cause cumulative damage that significantly reduces cell viability. Standard practice is to freeze tissue once and thaw only when needed. For this reason, tissue is often divided into multiple vials, allowing individual doses to be thawed while others remain frozen.
Q: How is DMSO removed after thawing?
A: Gradual dilution with isotonic saline solutions removes DMSO in stages. Multiple wash cycles slowly reduce DMSO concentration while allowing cells to rehydrate. This careful process prevents osmotic shock that could damage cells recovering from cryopreservation. The washing protocol is as important as the freezing protocol for preserving cell function.
Key Takeaways
Cryopreservation Science Validated protocols have been refined over decades of peer-reviewed research. The process addresses fundamental biological challenges of ice crystal formation and cellular dehydration through cryoprotectants and controlled-rate freezing.
Temperature Requirements Liquid nitrogen storage at negative 196°C provides theoretical indefinite preservation. The controlled freezing rate of negative one degree per minute is critical for preventing ice crystal damage.
Quality Control Matters Continuous monitoring, sterility testing, viability assessment, and CGTP compliance distinguish legitimate tissue banking from unregulated operations. Documentation and traceability are hallmarks of compliant services.
Post-Thaw Viability Studies document 80-91% cell viability after thawing from properly cryopreserved tissue. However, technical preservation success does not guarantee future therapeutic benefit, clinical trial eligibility, or any specific medical outcome.
Transparency Is Essential Understanding the science empowers you to ask informed questions. Legitimate tissue banking services openly discuss their protocols, quality measures, and limitations.
Ready to Learn More?
This educational content explains the science behind cryopreservation. It is not medical advice and does not guarantee future treatment access or outcomes. Discuss all medical decisions with qualified healthcare professionals.
Understanding cryopreservation science helps you make informed decisions about whether tissue banking aligns with your health planning goals. The validated protocols described here represent decades of research and real-world application.
Save My Fat provides adipose tissue banking using established cryopreservation methodology. Our focus is on transparency, validated science, and honest communication about what tissue banking can and cannot offer.
Questions about the cryopreservation process?
Contact Save My Fat to speak with our team about how tissue banking works. If you have medical questions about whether banking is appropriate for your situation, consult your physician.
Learn more about how stem cell banking works or explore emerging research in regenerative medicine.
Save My Fat Transparent Tissue Banking Based on Validated Science
Last updated: February 20, 2026