If you’re researching stem cell sources, one of the most common questions is whether adipose (fat) tissue or bone marrow provides a better source of mesenchymal stem cells. This guide compares the biological and practical characteristics of each source, covering cell yield, collection procedures, proliferation rates, differentiation potential, and safety profiles. By the end, you’ll understand how these two stem cell sources differ in measurable, science-backed ways, and what those differences mean for tissue banking decisions.
TLDR: Adipose tissue yields roughly 500 times more mesenchymal stem cells per volume than bone marrow and requires a less invasive collection procedure (15 to 30 minutes under local anesthesia vs. 30 to 60 minutes under general or spinal anesthesia). Adipose-derived cells also proliferate faster in culture and show minimal age-related decline. However, neither source has FDA-approved disease treatments based on cell source alone, and biological advantages do not automatically determine clinical outcomes. Read the full guide for detailed comparison data.
Critical Disclaimer: Biological vs. Clinical Comparison
This article compares the BIOLOGY of adipose-derived and bone marrow-derived stem cells only. It does NOT compare clinical efficacy for treating any disease. Both cell types remain investigational for most therapeutic applications. Neither has FDA approval for disease treatment based on cell source alone. Biological superiority in one measurable characteristic (such as cell yield or proliferation rate) does not determine whether one source will produce better clinical outcomes. This content is for educational purposes only and does not constitute medical advice. Patients must consult their own licensed healthcare professionals regarding all medical decisions.
You’ve probably heard that stem cells can come from bone marrow or from fat tissue, and you want to know: which one is actually better? It’s a natural question, and the answer depends entirely on what you mean by “better.” If you’re comparing raw cell numbers, collection ease, or how fast cells grow in the lab, the data points in clear directions. If you’re asking which source produces better treatment results for disease, the honest answer is that research is still working on that question.
The truth is that “better” in biology is context-dependent. Bone marrow and adipose tissue each have documented strengths in different areas. Understanding these real, measurable differences helps you ask smarter questions and avoid marketing claims that oversimplify the science. It also helps you evaluate whether adipose tissue banking aligns with your goals.
This guide walks through what the peer-reviewed research actually shows about each source’s biological characteristics, so you can distinguish scientific fact from promotional hype. Every data point cited here comes from published, peer-reviewed studies or authoritative regulatory sources.
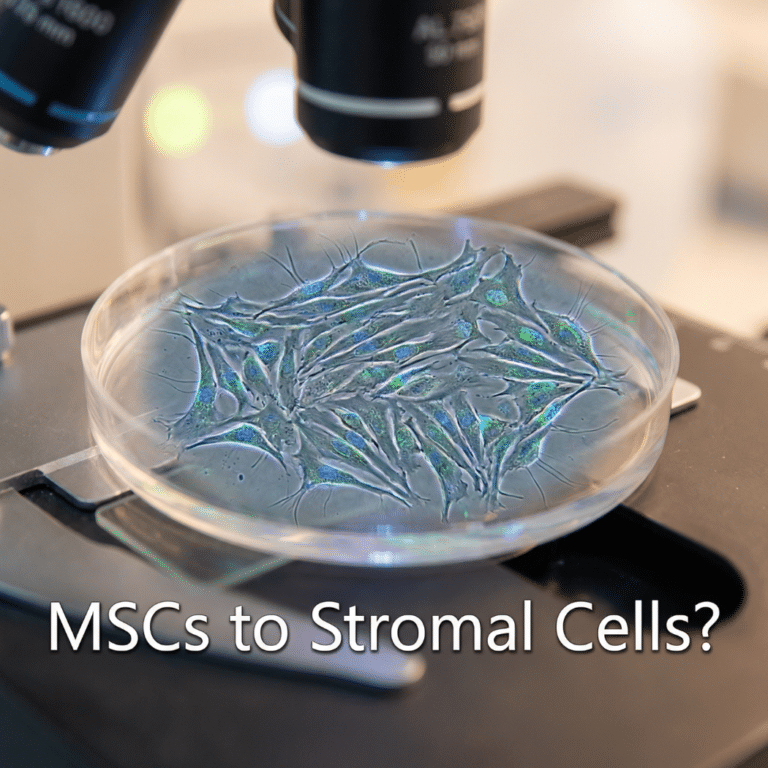
What Are Mesenchymal Stem Cells (MSCs)?
Mesenchymal stem cells (MSCs) are a type of adult stem cell found in multiple tissues throughout the body, including bone marrow, adipose (fat) tissue, umbilical cord tissue, dental pulp, and others. Unlike embryonic stem cells, which can become any cell type in the body, MSCs are multipotent, meaning they can develop into a limited number of cell types, primarily fat cells (adipocytes), bone cells (osteoblasts), and cartilage cells (chondrocytes).
The International Society for Cellular Therapy (ISCT) established three minimum criteria for classifying a cell as an MSC: the cells must adhere to plastic under standard culture conditions; they must express specific surface markers (CD73, CD90, and CD105) while lacking others (CD45, CD34, CD14, CD19, and HLA-DR); and they must demonstrate the ability to differentiate into fat, bone, and cartilage cells in the laboratory (Dominici et al., 2006, Cytotherapy).
Both adipose-derived MSCs and bone marrow-derived MSCs meet these ISCT criteria. They are the same general cell type, isolated from different tissue sources, with measurable differences in quantity, behavior, and practical characteristics that this guide explores in detail. Current research suggests MSCs exert their effects primarily through paracrine signaling (releasing beneficial molecules) rather than simply replacing damaged cells.
Collection Procedures: The Practical Difference
The collection procedure is one of the most significant practical differences between these two stem cell sources, and it directly affects patient experience, safety, and willingness to proceed.
Bone marrow aspiration requires penetrating bone (typically the posterior iliac crest at the back of the hip) under general or spinal anesthesia. The procedure takes 30 to 60 minutes and involves aspirating 50 to 100 mL of bone marrow through multiple needle insertions. A systematic review by Bain (2003, 2005) covering more than 19,000 bone marrow procedures documented adverse events in approximately 0.05 to 0.08% of cases, with hemorrhage as the most common serious complication and a mortality rate of approximately 0.002%. Pain is common: studies report that 60 to 70% of patients experience notable post-procedure pain, with a subset reporting severe discomfort lasting days to weeks.
Adipose tissue collection via liposuction is a minimally invasive outpatient procedure performed under local (tumescent) anesthesia. A small cannula (3 to 4 mm) aspirates 100 to 200 mL of fat tissue from the abdomen, flanks, or thighs in 15 to 30 minutes. A 2024 systematic review and meta-analysis covering 29,368 patients found an overall complication rate of 2.62%, with serious complications (infection at 0.02%, venous thromboembolism at 0.017%) occurring at extremely low rates (Comerci et al., 2024, Aesthetic Surgery Journal).
The following table summarizes these procedural differences:
| Parameter | Bone Marrow | Adipose Tissue | Advantage |
| Collection site | Posterior iliac crest | Abdomen, flanks, thighs | Adipose (accessible) |
| Anesthesia | General or spinal | Local (tumescent) | Adipose |
| Procedure duration | 30 to 60 minutes | 15 to 30 minutes | Adipose |
| Recovery time | 2 to 7 days | Same-day discharge | Adipose |
| Post-procedure pain | 60 to 70% report pain | Minimal | Adipose |
| Serious complications | 0.05 to 0.08% | Less than 0.1% | Comparable |
| Hospitalization | Sometimes required | Never required | Adipose |
| Patient burden | High | Low | Adipose |
For patients considering tissue banking, the collection experience is substantially easier with adipose tissue. Learn more about the adipose tissue collection process.
Cell Yield Comparison: The Numbers
Cell yield is where adipose tissue demonstrates its most dramatic measurable advantage. Published research consistently shows that adipose tissue contains a far higher concentration of mesenchymal stem cells than bone marrow.
In bone marrow, MSCs constitute only about 0.001 to 0.01% of all nucleated cells, equivalent to roughly 1 MSC in every 10,000 to 100,000 cells (Strioga et al., 2012, Stem Cells and Development). A standard harvest of 50 to 100 mL typically yields 0.5 to 2 million MSCs total, with significant variability based on donor age and health.
Adipose tissue, by contrast, contains a much higher frequency of stem cells. Studies report that 1 to 10% of the nucleated cells in the stromal vascular fraction (SVF) are adipose-derived stem cells, with yields of 300,000 to 570,000 cells per mL of processed tissue (Baer & Geiger, 2012, Stem Cells International). A typical harvest of 100 to 200 mL can yield 30 to 100 million stem cells after initial processing.
| Metric | Bone Marrow | Adipose Tissue | Advantage |
| MSC frequency | 0.001 to 0.01% of cells | 1 to 10% of SVF cells | Adipose (100x to 1,000x) |
| Cells per mL | Hundreds to low thousands | 300,000 to 570,000 | Adipose |
| Typical harvest volume | 50 to 100 mL | 100 to 200 mL | Similar |
| Yield per harvest | 0.5 to 2 million MSCs | 30 to 100 million cells | Adipose (50x to 100x) |
| After culture expansion | 1 to 5 billion potential | 5 to 10 billion potential | Adipose |
| Age effect on yield | Dramatic decline | Minimal decline | Adipose |
| Yield variability | Very high (age/donor) | Lower variability | Adipose |
This yield difference is a biological fact. However, higher cell yield does not automatically translate to better clinical outcomes. That question is separate and still under investigation. What the yield difference does mean practically is that fewer procedures and less culture time are needed from adipose tissue to reach therapeutically relevant cell numbers. For more on long-term preservation of these cells, see how cryopreservation works.
Biological Characteristics Compared
Beyond raw cell numbers, adipose and bone marrow MSCs differ in how fast they multiply, how long they can be expanded, and what cell types they most readily become.
Proliferation capacity: A landmark study by Kern et al. (2006, Stem Cells) directly compared MSCs from bone marrow, umbilical cord blood, and adipose tissue. Adipose-derived MSCs achieved approximately 17.2 cumulative population doublings by passage 5, compared to approximately 13.7 for bone marrow MSCs. Population doubling time for adipose MSCs is generally 24 to 48 hours, compared to 72 to 96 hours for bone marrow MSCs under comparable culture conditions, though exact times vary by media formulation, passage number, and donor factors.
| Parameter | Bone Marrow MSCs | Adipose MSCs | Advantage |
| Population doubling time | 72 to 96 hours | 24 to 48 hours | Adipose (2x to 4x faster) |
| CPD at passage 5 | ~13.7 doublings | ~17.2 doublings | Adipose |
| Total doublings before senescence | 30 to 40 | 50+ | Adipose |
| Time to therapeutic numbers | Longer | Shorter | Adipose |
| Expansion from single harvest | 1 to 5 billion | 5 to 10 billion | Adipose |
Differentiation potential: A rigorous donor-matched study by Mohamed-Ahmed et al. (2018, Stem Cell Research & Therapy) compared cells from the same nine donors to eliminate inter-individual variability. The results confirmed a clear pattern: adipose MSCs showed significantly superior adipogenic (fat cell) differentiation, with higher lipid formation and gene expression (p<0.001). Bone marrow MSCs demonstrated significantly superior osteogenic (bone cell) and chondrogenic (cartilage cell) differentiation, with earlier and higher alkaline phosphatase activity for bone and more cartilaginous matrix for cartilage.
| Lineage | Bone Marrow MSCs | Adipose MSCs | Stronger Source |
| Adipogenic (fat cells) | Moderate | Superior (95% at 2 weeks) | Adipose |
| Osteogenic (bone cells) | Superior | Comparable or reduced | Bone Marrow |
| Chondrogenic (cartilage) | Superior | Moderate, variable | Bone Marrow |
| Myogenic (muscle) | Limited | Limited | Comparable |
| Overall strength | Hard tissues | Soft tissues | Context-dependent |
Neither source is universally “better” for differentiation. Each has documented strengths in different lineages, which is consistent with their tissue of origin.
Donor Age Effects: A Critical Practical Factor
Age-related decline in stem cell yield and function is one of the most important practical differences between these two sources, and it strongly favors adipose tissue for patients over 40.
Bone marrow MSCs show a well-documented, dramatic decline with donor age. Stolzing et al. (2008, Mechanisms of Ageing and Development) demonstrated significant reductions in colony-forming unit counts, increased oxidative damage markers, and elevated cellular aging indicators (p21, p53) in older donors. Bone marrow cellularity itself declines from approximately 90% hematopoietic tissue at birth to roughly 50% by age 30 and approximately 30% by age 70 (Longo et al., 2009).
Adipose-derived MSCs, by contrast, show minimal age-related decline in total cell yield. While some studies note modest functional reductions in proliferation rate with advancing donor age, the overall yield and viability remain far more stable across the adult lifespan than bone marrow.
| Donor Age | Bone Marrow MSC Yield | Adipose ADSC Yield | Implication |
| Birth to 20 years | High | Very high | Both viable sources |
| 20 to 40 years | Moderate to high | High | Both viable sources |
| 40 to 60 years | Low to moderate | High | Adipose advantage |
| 60+ years | Very low | Moderate to high | Strong adipose advantage |
| Overall age dependence | Dramatic decline | Minimal decline | Adipose superior for older patients |
This age stability is a key reason why adipose tissue banking remains practical for adults across a wide age range. For details on long-term tissue storage, see how long adipose tissue can be stored.
Current Research Applications
Both cell sources are under active investigation across multiple medical specialties. Neither has broad FDA approval for disease treatment, but both have achieved important regulatory milestones.
Bone marrow MSCs have a longer research history, with the first isolation in the 1970s. In December 2024, the FDA approved Ryoncil (remestemcel-L), an allogeneic bone marrow-derived MSC product, for steroid-refractory acute graft-versus-host disease (GVHD) in pediatric patients. This represents the first FDA-approved mesenchymal stromal cell therapy in the United States.
Adipose-derived MSCs, while studied since the 1990s, have seen rapidly expanding clinical trial activity. As of mid-2024, more than 400 clinical trials investigating adipose-derived stem cell therapies were registered on ClinicalTrials.gov. In 2018, the European Commission approved Alofisel (darvadstrocel), an allogeneic expanded adipose-derived MSC product for complex perianal fistulas in Crohn’s disease. However, Alofisel was voluntarily withdrawn from the EU market in December 2024 after its confirmatory Phase 3 trial did not meet its primary endpoint. It remains approved in several other countries.
| Application Area | Bone Marrow MSCs | Adipose MSCs | Current Status |
| Osteoarthritis | Moderate research | Extensive (60+ trials) | Adipose more active |
| Bone regeneration | Extensive research | Moderate | Bone marrow preferred |
| Cartilage repair | Extensive research | Moderate | Bone marrow advantage |
| Crohn’s disease (fistulas) | Limited | Extensive (EU approval achieved, later withdrawn) | Adipose led historically |
| Wound healing | Moderate | Extensive | Adipose more active |
| GVHD | FDA approval (Ryoncil) | Limited | Bone marrow approved |
| Spinal cord injury | Active | Active | Both pursuing |
| Total registered trials | Substantial | 400+ on ClinicalTrials.gov | Adipose expanding faster |
Important: Neither adipose nor bone marrow MSCs have FDA-approved disease treatments based on cell source alone (Ryoncil’s approval is product-specific, not a blanket approval for bone marrow cells). Both cell types are investigational for most applications. Research activity does not equal proven clinical benefit.
Immunological Properties and Allogeneic Potential
Both MSC types offer a critical advantage for autologous (self-to-self) use: because the cells come from the patient’s own body, there is no risk of immune rejection and no need for immunosuppressive drugs. This is a significant safety advantage over allogeneic (donor-to-recipient) cell therapies and organ transplantation.
Both adipose and bone marrow MSCs also exhibit “immune-privileged” properties, meaning they express low levels of molecules that trigger immune rejection (low MHC Class I, no MHC Class II, no costimulatory molecules). This makes both sources potentially useful for allogeneic “off-the-shelf” products, as demonstrated by Ryoncil (bone marrow-derived, allogeneic) and historically by Alofisel (adipose-derived, allogeneic). Some comparative studies suggest adipose MSCs produce higher levels of certain immunomodulatory cytokines (such as IL-6, PGE-2, and IDO), but whether this translates to clinically meaningful differences remains under investigation.
Safety Profiles and Practical Considerations
Both cell types demonstrate excellent long-term safety records with no reported cases of teratoma (tumor) formation across thousands of clinical applications. A comprehensive safety meta-analysis covering 55 randomized controlled trials and 2,696 patients found no increased risk of malignancy from MSC therapy (Thompson et al., 2020, EClinicalMedicine/The Lancet). MSCs are multipotent, not pluripotent, meaning they lack the inherent capacity to form teratomas that pluripotent stem cells (embryonic and induced pluripotent) carry.
| Safety Factor | Bone Marrow MSCs | Adipose MSCs | Assessment |
| Collection invasiveness | High (bone penetration) | Low (liposuction) | Adipose safer |
| Teratoma risk | None documented | None documented | Equivalent (both safe) |
| Long-term malignancy | Excellent record | Excellent record | Equivalent |
| Post-procedure infection | 0.05 to 0.08% | Less than 0.1% | Comparable |
| Serious bleeding | Documented (hemorrhage) | Not reported | Adipose safer |
| Recovery time | 2 to 7 days | Same day | Adipose faster |
| Anesthesia required | General or spinal | Local only | Adipose lower risk |
Both cell sources can be safely cryopreserved for long-term storage using validated protocols. Neither has shown concerning safety signals in extended follow-up studies spanning two or more years.
Practical Comparison for Banking Decisions
When the comparison shifts from pure biology to practical banking considerations, the differences become clearer. The following table summarizes the factors most relevant to patients considering tissue preservation.
| Factor | Bone Marrow | Adipose Tissue | For Banking |
| Ease of collection | Difficult, invasive | Simple, outpatient | Adipose preferred |
| Patient burden | High (pain, recovery) | Low (minimal discomfort) | Adipose preferred |
| Cell yield per procedure | 0.5 to 2 million MSCs | 30 to 100 million cells | Adipose preferred |
| Expansion potential | Lower, slower | Higher, faster | Adipose preferred |
| Age-related decline | Severe | Minimal | Adipose preferred |
| Time to therapeutic numbers | Longer | Shorter | Adipose preferred |
| Suitable for older adults | Limited by declining yield | Excellent across ages | Adipose preferred |
| Established FDA product | Yes (Ryoncil for GVHD) | Emerging | Bone marrow precedent |
| Overall banking choice | Rarely chosen for banking | Most commonly banked | Adipose preferred |
Readers must understand: adipose tissue yields more cells, is less invasive to collect, and expands faster in culture. These are measurable biological facts. Whether these advantages translate to better clinical outcomes for any specific disease is a separate question that research has not yet answered definitively. Both cell types are still being studied for most therapeutic applications.
Frequently Asked Questions
Q: What’s the actual difference between adipose and bone marrow stem cells?
Both are mesenchymal stem cells (MSCs) that meet the same ISCT classification criteria. The key differences are practical and biological: adipose tissue yields roughly 500 times more MSCs per volume, requires less invasive collection, and shows minimal age-related decline. Bone marrow MSCs have a longer research history and may have advantages for bone and cartilage differentiation. For more details, visit our FAQ page.
Q: Is one type biologically “better” than the other?
Neither is universally better. Adipose MSCs proliferate faster, yield more cells per harvest, and show superior fat cell differentiation. Bone marrow MSCs demonstrate stronger bone and cartilage differentiation in laboratory studies. “Better” depends entirely on the specific biological characteristic being measured.
Q: Does higher cell yield mean better treatment results?
Not necessarily. Higher yield means fewer procedures and less culture time are needed to reach target cell numbers, which is a practical advantage. However, whether more cells equals better clinical outcomes is a separate research question that has not been definitively answered. Clinical efficacy depends on many factors beyond cell count.
Q: Which harvest procedure is safer?
Adipose tissue collection via liposuction has a more favorable safety profile: local anesthesia, 15 to 30 minutes, same-day discharge, and very low complication rates. Bone marrow aspiration requires general or spinal anesthesia, bone penetration, and carries higher pain burden and complication risk. Both are considered medically safe when performed properly.
Q: Can both types be cryopreserved for future use?
Yes. Both adipose-derived and bone marrow-derived MSCs can be safely cryopreserved using validated protocols while maintaining viability and function. Adipose tissue can also be cryopreserved as whole tissue (without cell isolation), providing additional flexibility for banking.
Q: Do these biological differences matter for tissue banking?
Yes, significantly. Adipose tissue’s higher yield, easier collection, faster expansion, and age stability make it the preferred source for tissue banking. One adipose harvest can provide enough cells for multiple future uses, while bone marrow’s lower yield and age-dependent decline limit its banking practicality, especially for patients over 40.
Q: Are there FDA-approved treatments using either cell type?
As of early 2026, Ryoncil (remestemcel-L), a bone marrow-derived MSC product, received FDA approval in December 2024 for pediatric steroid-refractory acute GVHD. This is the first and currently only FDA-approved MSC product in the United States. No adipose-derived MSC product currently holds FDA approval for disease treatment. Banking tissue today does not guarantee access to future approved therapies.
Q: Why would someone choose to bank adipose tissue specifically?
Patients choose adipose tissue banking because of its practical advantages: the collection is minimally invasive, yields are high regardless of age, cells expand efficiently in culture, and cryopreservation can preserve tissue for potential future use in FDA-regulated clinical research, Expanded Access programs, or approved therapies. Banking does not guarantee future treatment access or clinical benefit.
Key Takeaways
Cell Yield: Adipose tissue yields roughly 500 times more mesenchymal stem cells per volume than bone marrow. This is the most dramatic measurable difference between the two sources, supported by multiple peer-reviewed studies.
Collection: Adipose tissue collection is faster (15 to 30 minutes vs. 30 to 60 minutes), less invasive (local vs. general/spinal anesthesia), and carries lower patient burden. Both procedures have acceptable safety profiles.
Proliferation: Adipose MSCs proliferate 2 to 4 times faster than bone marrow MSCs and maintain proliferative capacity longer in culture, reaching therapeutic cell numbers more efficiently.
Differentiation: Adipose MSCs excel at fat cell differentiation. Bone marrow MSCs excel at bone and cartilage differentiation. Neither is universally superior.
Age: Adipose tissue shows minimal age-related decline in MSC yield, making it viable for adults of any age. Bone marrow MSC yield declines dramatically with age, limiting its utility for older patients.
Safety: Both sources have excellent safety records with no teratoma formation reported across thousands of procedures. MSC therapy meta-analyses show no increased cancer risk.
Critical Caveat: Biological advantages (more cells, faster growth, easier collection) do not automatically mean better clinical outcomes. Both cell types remain investigational for most therapeutic applications, and neither source has broad FDA approval for disease treatment.
Ready to Learn More About Adipose Tissue Banking?
You now understand the measurable biological and practical differences between adipose-derived and bone marrow-derived mesenchymal stem cells. The data consistently shows that adipose tissue offers practical advantages in cell yield, collection ease, proliferation speed, and age stability, making it the preferred source for tissue banking.
Save My Fat helps individuals preserve adipose tissue through validated cryopreservation protocols for potential future use in FDA-regulated clinical research, Expanded Access programs, or approved therapies. We focus on education, scientific accuracy, and honest communication about both possibilities and limitations.
Ready to learn more? Visit savemyfat.com or explore our frequently asked questions for additional information about the tissue banking process.
Before You Contact Us: Adipose tissue banking is a preservation service for potential future opportunities, not a treatment or cure for any disease. Outcomes cannot be guaranteed. All medical decisions must be made with your licensed healthcare provider. Banking does not guarantee access to any therapy, clinical trial, or Expanded Access program.
References
- Dominici M, et al. “Minimal criteria for defining multipotent mesenchymal stromal cells.” Cytotherapy. 2006;8(4):315-317. PMID: 16923606.
- Strioga M, et al. “Same or not the same? Comparison of adipose tissue-derived versus bone marrow-derived MSCs.” Stem Cells Dev. 2012;21(14):2724-52. PMID: 22468918.
- Baer PC, Geiger H. “Adipose-derived mesenchymal stromal/stem cells: tissue localization, characterization, and heterogeneity.” Stem Cells Int. 2012;2012:812693. PMID: 22577397.
- Kern S, et al. “Comparative analysis of mesenchymal stem cells from bone marrow, umbilical cord blood, or adipose tissue.” Stem Cells. 2006;24(5):1294-1301. PMID: 16410387.
- Mohamed-Ahmed S, et al. “Adipose-derived and bone marrow mesenchymal stem cells: a donor-matched comparison.” Stem Cell Res Ther. 2018;9(1):168. PMID: 29921311.
- Bain BJ. “Bone marrow biopsy morbidity and mortality.” Br J Haematol. 2003;121(6):949-51. PMID: 12786808.
- Bain BJ. “Bone marrow biopsy morbidity: review of 2003.” J Clin Pathol. 2005;58(4):406-8. PMID: 15790706.
- Comerci G, et al. “Risks and complications rate in liposuction: a systematic review and meta-analysis.” Aesthet Surg J. 2024. PMID: 38563572.
- Stolzing A, et al. “Age-related changes in human BM-MSCs: consequences for cell therapies.” Mech Ageing Dev. 2008;129(3):163-173. PMID: 18241911.
- Longo DL, et al. “Bone marrow, thymus and blood: changes across the lifespan.” Aging Health. 2009;5(3):385-393. PMC: PMC2805199.
- Thompson M, et al. “Cell therapy with intravascular administration of MSCs continues to appear safe.” EClinicalMedicine. 2020. PMID: 31989101.
- FDA. “FDA Approval of Ryoncil (remestemcel-L-rknd).” December 18, 2024. FDA.gov.
Save My Fat Adipose Tissue Banking for Future Regenerative Medicine Opportunities
Last updated: February 24, 2026